

A New Diagnostic Flow
An conversation with Dr. Christine Metz on diagnosing endometriosis without surgery

What if it took open heart surgery to know if you had high blood pressure?
That’s what it can feel like for 1 in 10 people in the world with a uterus who might have “endometriosis”: a common, painful chronic disease that causes inflammation, infertility, and severe menstrual pain… and they might not even know they have it.
Roughly 190 million worldwide struggle with the once-overlooked disease.1
Dr. Christine Metz, a professor at Northwell Health and the Donald and Barbara School of Medicine, is on a mission to change that.

Source: Northwell Health
I spoke with her for Grand Technologies where I look at how technology impacts our daily lives. Her work stands to improve the lives of millions, but that impact did not happen overnight. It takes a patient and curious mindset to pioneer research in a field, a journey that can take decades before blooming results to innovate new technology.
“That pain is normal.”
As endometriosis lesions grow, they causes inflammation, which can lead to adhesions, scarring, internal bleeding, bowel or urinary dysfunction, constipation, painful intercourse, and infertility. The physical pain can be severe, which can lead to psychological distress. It’s a combination that, in many ways, can have a debilitating effect on an individual’s life. - Endometriosis Foundation of America.2
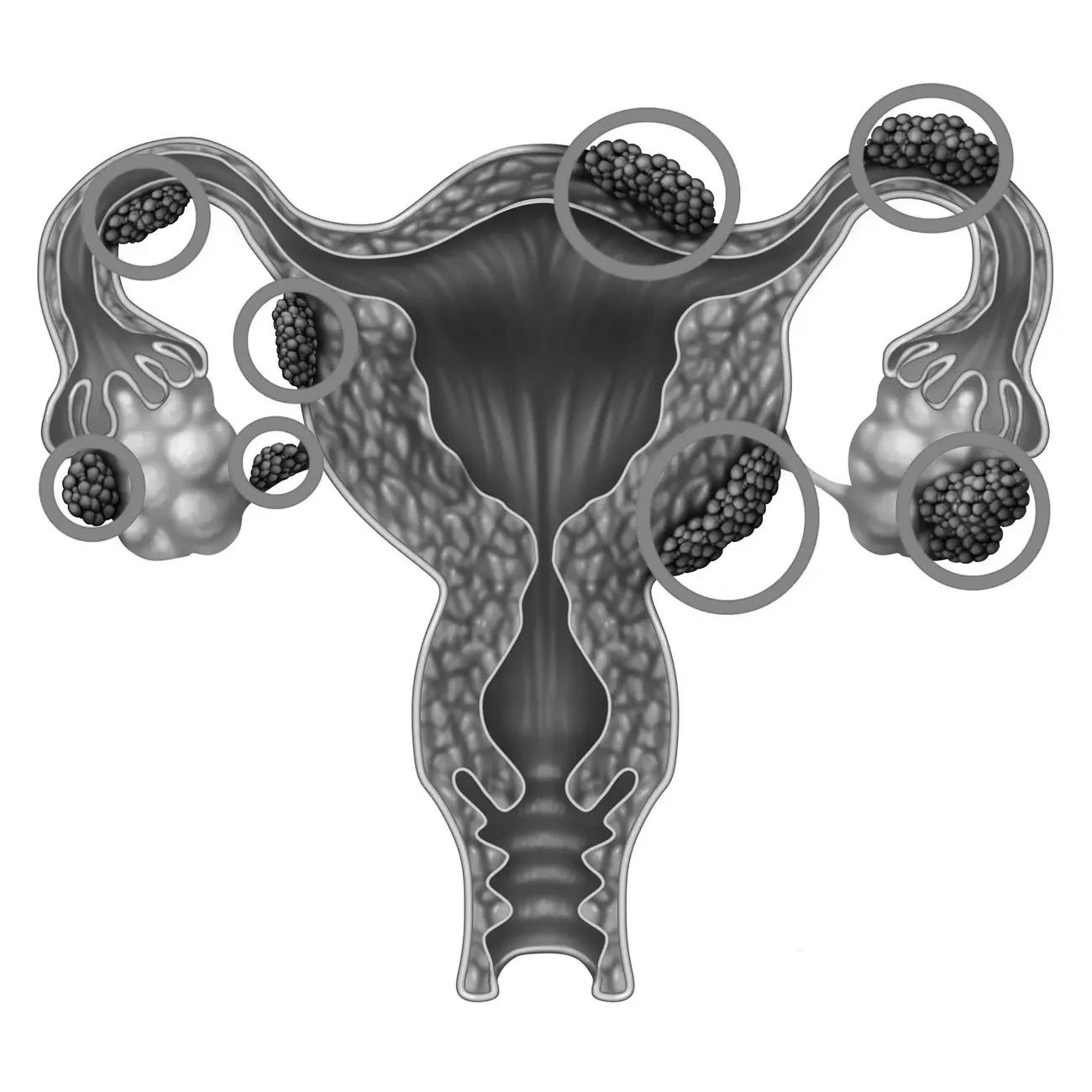
Source: wildpixel/Getty Images
The disease’s debilitating pain goes unnoticed, requires a surgery to diagnose, and lacks effective treatment.
It started with the hiccups: in the eighth grade, for a month straight, Cate Gogolak found herself hiccuping with alarming frequency. Next came acid reflux, bowel issues, and frequent urination. During her freshman year of high school, she experienced a weird pulling sensation, as if someone were reaching into her abdomen and trying to drag her uterus out of her body. The feeling seemed to get worse during her period. Her mother took her to see a range of specialists, but the tests all came back negative. - New Yorker3
The pain that marks endometriosis usually begins early, even before puberty for some, which makes diagnosis difficult.
Dr. Metz notes that, “About 70% of patients with moderate to severe endometriosis claim their symptoms started when they were teens. It usually starts early and it progresses.”
That pain is normalized in part because doctors face a high hurdle to diagnose endometriosis. They may pursue other diagnoses that match some symptoms or prescribe antidepressants as frontline medication (New Yorker).
Also at play is broader stigmatization of women’s health that undermines correctly diagnosing endometriosis— and developing approaches to treat it. The “yuck factor” has made open conversations harder. Sex education in some states, like Florida, has been severely restricted. Entire districts cancel classes rather than risk violating new state guidelines.4
Normalization of pain and dismissal of pain are all too common. Dr. Metz says it’s made worse by age - “the younger you are, dismissal seems too frequent and more serious.”
“Knowing will require surgery.”
Let’s say a doctor doesn’t dismiss your symptoms and seeks to confirm endometriosis… Dr. Metz notes the diagnostic journey might start with “imaging methods, ultrasound or MRI, they require the lesions to be quite large to be detected. So, it is unlikely the patient will be diagnosed in their teens, for example, when their debilitating symptoms begin.
But the definitive gold standard is a “laparoscopy”, an invasive surgery that begins with small incisions in the abdomen, followed by inserting a small camera; if surgeons find lesions, they remove them so a pathologist can confirm the presence of what Dr. Metz calls “uterine-like” cells, i.e., endometriosis.
After surgery, relief is far from guaranteed. Up to 80% will experience pain again within two years because some endometriosis tissue was either not visible or could not be removed, according to the American College of Obstetricians and Gynecologists.5
After diagnosis and the initial relief of surgery, ongoing treatment involves hormone-based medications like birth control with varying outcomes. Dr. Metz talks about how understudied the treatment options are, “[hormones are] a common treatment for many conditions affecting women. Hormone treatments are not a common treatment for men’s conditions. Some physicians I’ve spoken to believe that hormones may make some people with endometriosis experience worse symptoms.”
The journey for anyone facing endometriosis is brutal. The pain is normalized or dismissed. Diagnosis is costly and delayed. Treatment has been understudied and often ineffective. Outcomes vary.
The ROSE begins to bloom
The innovative technology we rely on often emerges out of researchers tinkering and toiling in labs for decades.
This research venture did not come out of a pitch deck in Silicon Valley, it came from two scientists at a Long Island research institute bucking the trend. Dr. Metz’s contributions have not happened overnight, “I had been working on endometriosis for many years prior to that, since the late 1990s, with a collaborator in Quebec who was very interested in the inflammatory aspects of endometriosis.
It wasn’t until 2012 that an innovative diagnostic approach arose thanks to research elsewhere describing differences in the cells lining the uterus in patients with endometriosis compared to healthy people.
A year later, Peter Gregersen, MD, and Christine Metz, PhD earned a grant through the Endometriosis Foundation of America to start collecting biological specimens to study endometriosis. This launched the “ROSE” study. Research OutSmarts Endometriosis to enroll teens and women who are healthy, are diagnosed with endometriosis, or exhibit symptoms, but are not yet diagnosed, to donate their menstrual blood, containing shed uterine tissue, for research.
When the team started, there were serious doubts about whether collecting menstrual blood would provide useful information, like stool and urine. Dr. Metz notes the resistance from physicians, “I attended the first menstruation meeting at the NIH before the pandemic. Several people laughed. We had kind of a cold reception from some. When we asked gynecologists to help recruit from their patient populations, many told us that they did not feel comfortable asking their patients to provide menstrual blood for a study.”6 Instead, doctors would say, “I know endometriosis when I see it.”
Since 2013, the stigma to provide menstrual blood has slowly started to erode thanks to social media, press, and word of mouth. Dr. Metz recounts, “there was some social media growth. And we had a couple of participants in our study who shared their journeys on social media. There was also a New York Times article that featured endometriosis and the ROSE study. And we experienced a flood of participants willing to share their menstrual blood.”
The ROSE Study has grown to more than 3,700 participants. Today, Dr. Metz says the study has taken off, “It’s no longer a challenge for us to recruit participants, either through social media or word of mouth.” And thanks to advances in technology, researchers can obtain more insights out of every drop of blood donated.
The Breakthrough: A New Diagnostic Flow
Instead of an invasive surgery, the ROSE team samples the uterus performing, in a sense, its own natural biopsy— menses, the beginning of the menstrual cycle.
For years, the ROSE team processed menstrual blood by separating out the liquid portion to analyze the free cells. Then a gap-year medical student working in the lab kept asking a question no one had thought to ask. Dr. Metz recalled her thinking at the time, “What’s in this “meat” portion that we throw away?”
They went back and looked. There were clear, large pieces of intact tissue — not dead cells, not trash, but living endometrial tissue. Dr. Metz recalls the buzz in the lab, “The endometrium has to shed and regrow every single month. So, of course, the menstrual blood is full of live intact uterine tissues. And we had been throwing them away.” That changed the study’s trajectory.

The team could now feed the mRNA data from those cells alongside patient profile information into machine learning algorithms. “There are very few reports that characterized menstrual blood in a meaningful way.” This is changing that to provide a “risk score” to predict the presence of endometriosis without surgery.
The innovation boils down to a score the physician can discuss with the patient to decide ‘next steps’, derived from something the uterus produces every month.
Collecting the data requires what Dr. Metz describes as a “novel menstrual collection device”. Current tampons and pads kill cells on arrival. Instead, an at-home menstrual collection that is sent to a central lab for diagnostic analyses is in the works for eventual FDA review and approval.
Today
Today, ROSE is 3,700 strong. “Everything can be done at home, which is great because we’re able to recruit menstruators from North America. We are interested in identifying young people who are suffering so they can get early treatment and perhaps more preventative care in the future.” And the research opens up new paths, “We are applying this technology to menstrual effluent collected from endometriosis patients, as well as menstrual effluent collected from patients with infertility. There are multiple other uterine health conditions we could study.
Hurdles remain with where the work needs to go. The “yuck factor” of period blood stigmatizing testing prevents diagnosing potential patients in pain and doctors feeling comfortable doing so. Earning FDA approval for at-home collected menstrual blood to be used for diagnostic purposes is a challenge, says Dr. Metz, “COVID sparked the development of ‘at-home’ biospecimen collections for downstream diagnostics and testing. ”Scaling the research to provide a diagnostic approach that reaches more people in pain requires starting a company. Dr. Metz also notes the challenges in keeping up funding to expand the study to analyze more samples, “as academics, it’s difficult to get funding required to do this at scale and to address all the regulatory issues.”
Lots of work remains for Dr. Metz and the ROSE team to improve diagnosing and treating endometriosis. Her enthusiasm for the work is well-timed; funding for women's health startups is accelerating. Since 2020, femtech startups have raised over $5 billion in venture capital with $1.2 billion in 2024 alone, a 20% increase from the prior year, according to PitchBook data.7 More capital brings in more partners from the private sector to make the ROSE team’s job easier to free patients and physicians stuck in an analysis paralysis.
For Dr. Metz, the journey of ROSE has been long and is beginning to bloom into new technology. To learn more and get involved in the study, visit the ROSE website online.
“Endometriosis,” World Health Organization (March 24, 2023). https://www.who.int/news-room/fact-sheets/detail/endometriosis
“Endometriosis,” Endometriosis Foundation of America. https://www.endofound.org/endometriosis
Rachel Aviv, “What Can We Learn from Menstrual Blood?” The New Yorker (September 9, 2024). https://www.newyorker.com/magazine/2024/09/09/what-can-we-learn-from-menstrual-blood
Leslie Postal, “Emphasize abstinence in sex ed, Florida tells schools, skip contraception,” Orlando Sentinel (September 22, 2024). https://www.orlandosentinel.com/2024/09/22/emphasize-abstinence-in-sex-ed-florida-tells-schools-skip-lessons-on-contraception/
“Endometriosis,” American College of Obstetricians and Gynecologists. https://www.acog.org/womens-health/faqs/endometriosis
“How Your Tampon Could Help Diagnose Endometriosis,” Bustle. https://www.bustle.com/wellness/menstrual-blood-tampon-studies-endometriosis-nextgen-jane
“FemTech VC Market Snapshot 2025,” PitchBook (2025). https://pitchbook.com/news/reports/2025-femtech-vc-market-snapshot